
COVID-19 isn’t just a respiratory disease: It can silently attack the heart. New research shows the virus accelerates plaque buildup in the arteries, increasing the risk of heart attacks and strokes long after recovery.
A new study has found that COVID-19, caused by the SARS-CoV-2 virus , is associated with a faster buildup of plaque in the coronary arteries, which increases the risk of heart-related complications. The findings were published today (Feb. 4) in Radiology , the journal of the Radiological Society of North America (RSNA).
“COVID-19, caused by SARS-CoV-2, is initially characterized by acute lung injury and respiratory failure,” explained senior study author Dr. Junbo Ge, professor and director of the Department of Cardiology at Zhongshan Hospital of Fudan University in Shanghai, China. “However, emerging evidence suggests that COVID-19 is also associated with an extreme inflammatory response that can affect the cardiovascular system.”
Long-term consequences of inflammation
This inflammation persists beyond the first month of infection, increasing the risk of serious cardiovascular problems and even death, Dr. Ge notes.
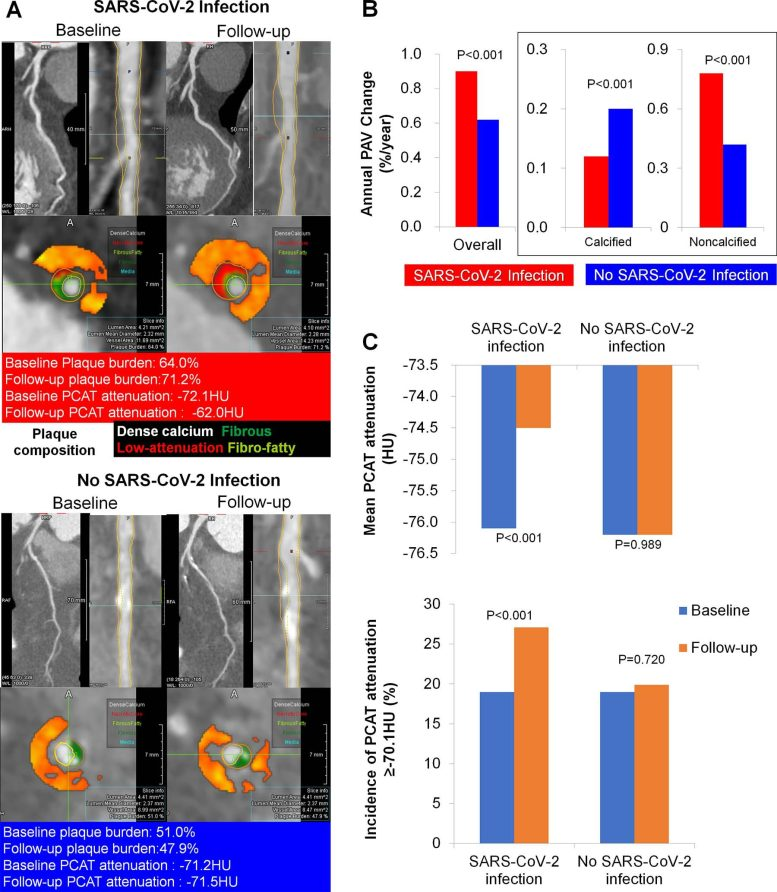
To understand this effect, researchers used coronary CT angiography (CCTA) to examine changes in the tissue surrounding the coronary arteries. They looked at markers of inflammation, plaque buildup and the presence of high-risk arterial blockages.
The retrospective study included patients who underwent CCTA between September 2018 and October 2023. The final study cohort consisted of 803 patients (mean age, 63.9 years; 543 men), including 329 patients (41%) who underwent imaging before the COVID-19 pandemic and 474 patients who underwent imaging during the pandemic. Of these, 25 patients were infected with SARS-CoV-2 prior to imaging.
Plaque development and high-risk lesions
The research team analyzed a total of 2,588 coronary artery lesions, including 2,108 lesions in patients with SARS-CoV-2 and 480 lesions in uninfected patients.
For all patients, the researchers compared baseline and follow-up measurements for plaque volume change, presence of high-risk plaque, and inflammation. They also analyzed the relationship between SARS-CoV-2 and cardiovascular events, such as heart attacks or revascularization procedures.
Increased risk of heart attacks and strokes
At baseline, mean arterial stenosis per lesion was 31.3%. Only 8.1% of lesions had a diameter stenosis of 50% or more.
Compared with uninfected patients, plaque volume increased more rapidly in patients infected with SARS-CoV-2. Lesions in patients infected with SARS-CoV-2 had a higher rate of progression to high-risk plaque (20.1% vs. 15.8%) and coronary arteritis (27% vs. 19.9%). Patients with COVID-19 also had a higher risk of target failure (10.4% vs. 3.1%), an indicator of increased risk of heart attack or stroke.
“Post-COVID-19 inflammation may lead to continued plaque growth, especially in high-risk noncalcified plaques,” Dr. Ge said. “Patients infected with SARS-CoV-2 are at increased risk of myocardial infarction, acute coronary syndrome, and stroke for up to one year.”
Need for long-term cardiovascular follow-up
These effects persisted after COVID-19, regardless of comorbidities such as age, hypertension and diabetes, he added.
“It is imperative to have effective treatment strategies for these patients,” said Dr. Ge.
The findings suggest that SARS-CoV-2 infection may exacerbate cardiovascular risk by accelerating the progression of vulnerable plaques and inflammation in coronary arteries. However, a more complete understanding of the biological mechanisms is needed to develop preventive and therapeutic approaches.
“It is important to anticipate that the burden of cardiovascular patients will be higher in the future as most infected individuals recover from acute SARS-CoV-2 infection,” said Dr. Ge.
Reference: “The relationship between SARS-CoV-2 infection and atherosclerotic plaque progression on CT coronary angiography and adverse cardiovascular events” by Drs. Ge, Neng Dai, MD, Xianglin Tang, MD, Yiqing Hu, MD, Hao Lu, MD, Zhangwei Chen, MD, Shaofeng Duan, PhD, Weifeng Guo, MD, Pranav Prakash Edavi, MD, Yongfu Yu, PhD, Dong Huang, MD and Juying Qian, MD Radiology .

